
Hone your POCUS interpretation and clinical reasoning by working through the interactive cases below.
Case #9: RV There yet??
Ms. RV is a 88 year old female with diastolic dysfunction and severe mitral regurgitation who is presenting with dyspnea and anasarca
Initially, she was hypotensive (BP 80/50), with peripheral cyanosis, in atrial fibrillation with a heart rate of 100-130, requiring 4L O2 to maintain oxygen saturation of 98%
She also had a Cr ~400 (baseline Cr 150), BNP 18,000, and troponin 41
CXR did not demonstrate significant evidence of pulmonary edema
You begin your POCUS assessment with imaging of the left and right lungs.
Left Lung Views
Right Lung Views
You move on to the parasternal long and short axis views.
Parasternal Long Axis
Parasternal Short Axis
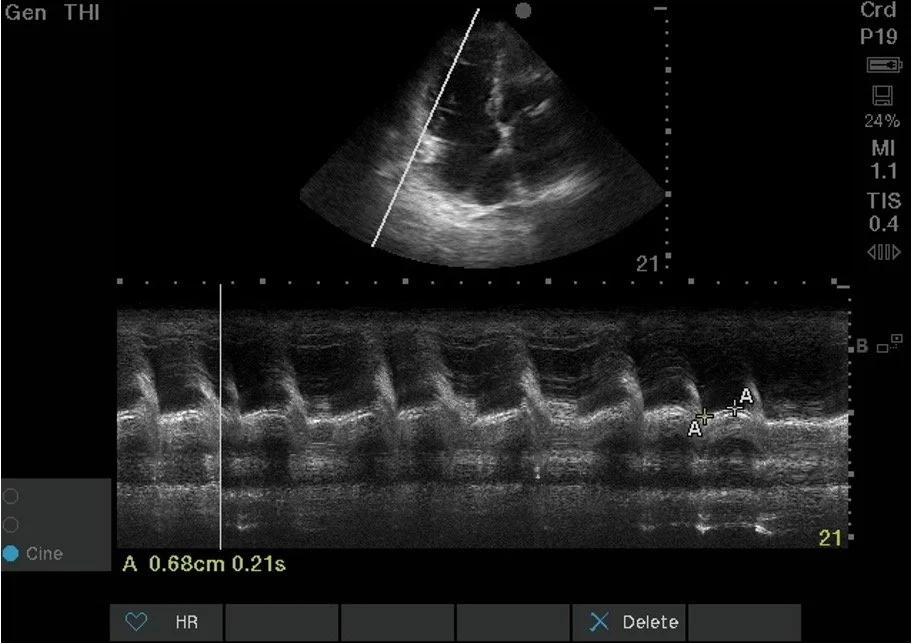
Next, you obtain an apical four chamber view and measure the TAPSE.
Apical Four Chamber
The next images you obtain are of the IVC.
IVC Sagittal Axis
IVC Transverse Axis
Onto colour doppler imaging.
Apical Four Chamber with Colour
Finally, you assess venous congestion using VExUS.
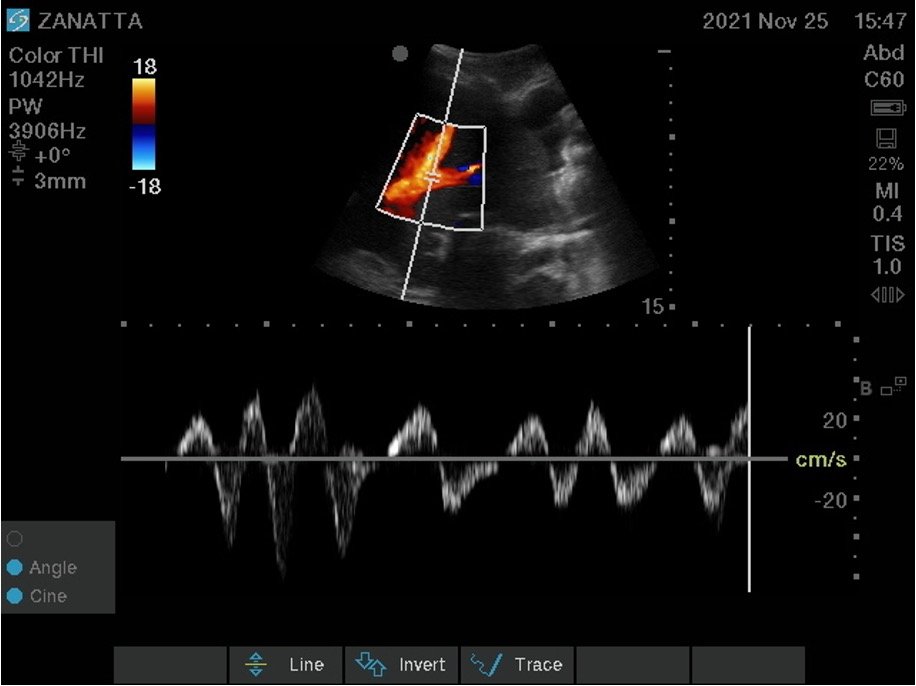
VExUS Hepatic Vein
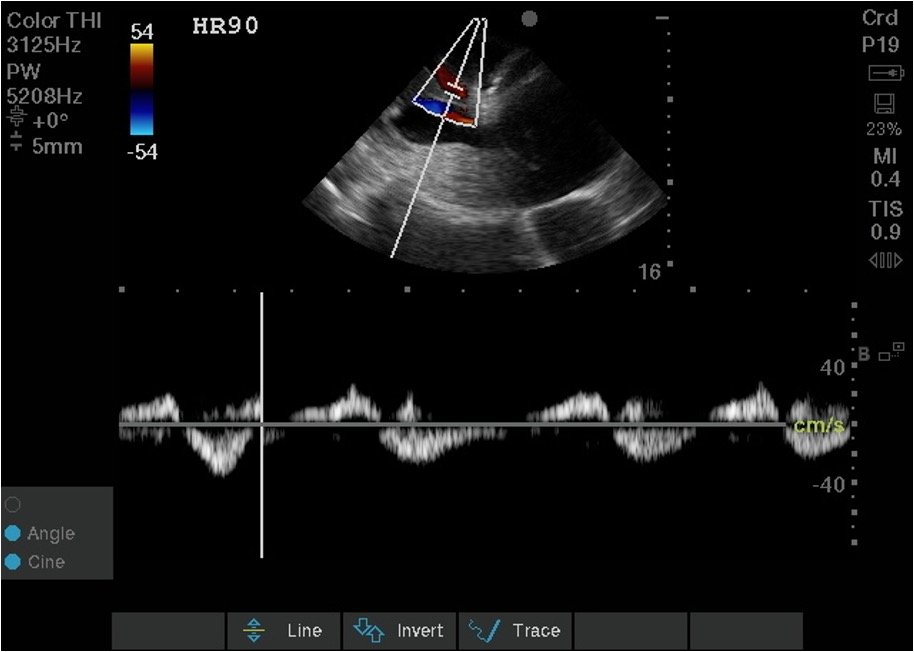
VExUS Portal Vein
Back to the case. How will you manage this patient?
Case Conclusion
The patient was started on a lasix infusion with metolazone
Midodrine was started for BP support as she was not a candidate for ICU
Her BP improved to 120/80 and Cr returned to her baseline with diuresis!
Ultimately, due to her end-stage heart failure and persistently low GCS, she was made comfort care
POCUS Pearls
RV enlargement is defined by RV size (at the tricuspid annulus) >⅔ the size of the LV (at the mitral annulus) severe is defined by RV size > LV size
RV pressure overload is defined by septal flattening in systole and RV volume overload is defined by septal flattening in diastole
Management of RV failure includes diuresis, selective pulmonary vasodilators (epoprostenol, nitric oxide), inotropes (milrinone, dobutamine), and treating the underlying cause if possible.