

Hone your POCUS interpretation and clinical reasoning by working through the interactive cases below.
Case #4: elevated creatinine of unclear duration
This was a 56-year old previously healthy gentleman who presented with a markedly elevated creatinine at 693 umol/L.
He had been sent in to the ED from his GP after outpatient lab work - he had presented to the clinic with a 2-week history of nausea, epigastric pain, and decreased appetite. He had been hypertensive in the clinic at 170/90; there were no previous BP measurements or lab works over the past 15 years. On further questioning, he denied any urinary symptoms; he wakes up once per night to urinate, but has no other LUT symptoms. Rheumatologic and infectious ROS are negative. His social history is unremarkable with no exposures, illicit substance use, or STI risk factors. Family history reveals a brother with “kidney issues.”
On physical exam, vitals are a BP of 172/96, HR 105, RR 18, 98% on RA, 36.8C. He appears well. Cardiac, respiratory, and abdominal exams are unremarkable. JVP does not appear elevated. Neuro exam is normal, and there are no rashes or active joints.
Relevant labwork includes a normocytic anemia with a Hgb of 93; platelets and WBC and normal. Electrolyte profile shows Na+ 141, K+ 4.9, HCO3- 21, Cl- 115, Cr 691, urea 28.7. Phosphate is 1.54mmol/L (elevated) and ionized calcium is 1.26 mmol/L (normal). Liver enzymes, albumin, CK, CRP, INR/PTT, TSH, EKG and CXR are all normal. Urinalysis shows trace protein, hemoglobin, and leukocytes; urine microscopy is pending.
The bladder was scanned to assess for the source of distal obstruction:


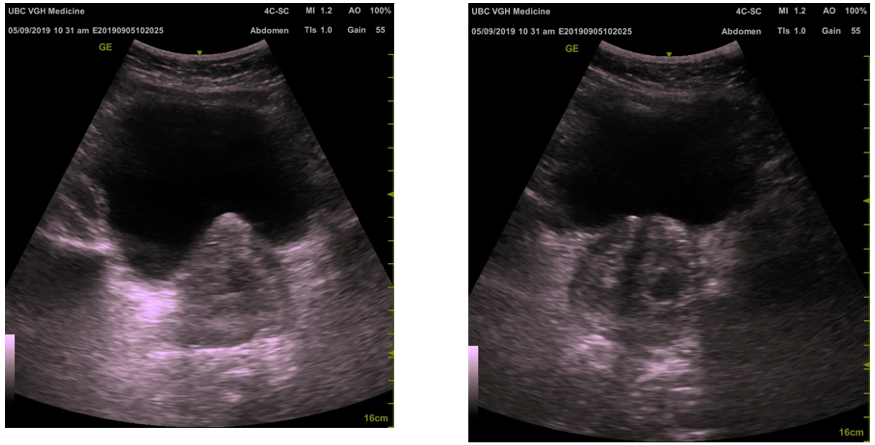
Enlarged prostate ~ 80 cc (normal < 25cc).
Additional Information
Both the bladder and prostate volume can be calculated using the ellipsoid formula
The cranial to caudal dimension and anterior to posterior dimension are measured in millimetres in the long axis view (sagittal plane of the body)
The width of the structure is measured in millimetres the short axis (transverse plane of the body)
the volume can then be calculated by multiplying the product of the 3 dimensions by 0.52

Further Laboratory Investigations
SPEP normal, no monoclonal band
Hepatitis B sAg/sAg/cAb negative, Hepatitis C Ab negative, HIV negative
ASOT negative
ANA, ANCA, anti-GBM negative
C3 normal, C4 0.38 (normal 0.12-0.36g/L)
PSA 12 (normal <3.5mcg/L)
Ferritin 269, TIBC 52, Tsat 17% (normal 20-55%), iron 9
U/A mild protein, large hemoglobin, moderate leukocytes
Urine Microscopy: Occassional hyaline and granular casts, moderate RBCs and WBC
Case Conclusion
Foley placed
drained clear urine (~2L over 12hrs)
Creatinine trend
24 hrs post foley insertion 550 - 48hrs 510 - 480 (D/C)
Started on Tamsulosin and Dutasteride prior to D/C
D/C with indwelling foley to be seen by Urology in 2 - 3d
As outpatient became Cr came down to 300’s ~1 wk post d/c
Ultimately, there was felt to be a component of delayed renal recovery secondary to prolonged hydronephrosis as well as possible component of pre-renal/post obstructive diuresis.