
Hone your POCUS interpretation and clinical reasoning by working through the interactive case below.
Case #13: It’s Draining Men!
Written by Lucia Juehea Lee and Lorena Mota-Lopez
Mr. T is a 62M with a history of type 2 diabetes, chronic kidney disease (Stage 3A), discoid lupus and possible connective tissue disease (?Sjogren’s).
He had a recent admission to the hospital for a fall (sustained a month ago) in the context of a diabetic foot infection and polymicrobial bacteremia. During this admission, he had a CT chest that reported multiple subacute right sided rib fractures with corresponding large right pleural effusion, “presumably hemothorax”. For this, he underwent a pigtail catheter insertion 2 weeks ago which drained serous, yellow fluid. Unfortunately, his pigtail fell off after draining 250cc and his fluid was never sent for analysis. Patient self-initiated his discharge against medical advice a 2 days later.
He returned to care due to worsening dyspnea, productive cough and right-sided pleuritic chest pain. There was no fevers and white cell count was normal. Hgb dropped from baseline 70-80s to 66 g/L.

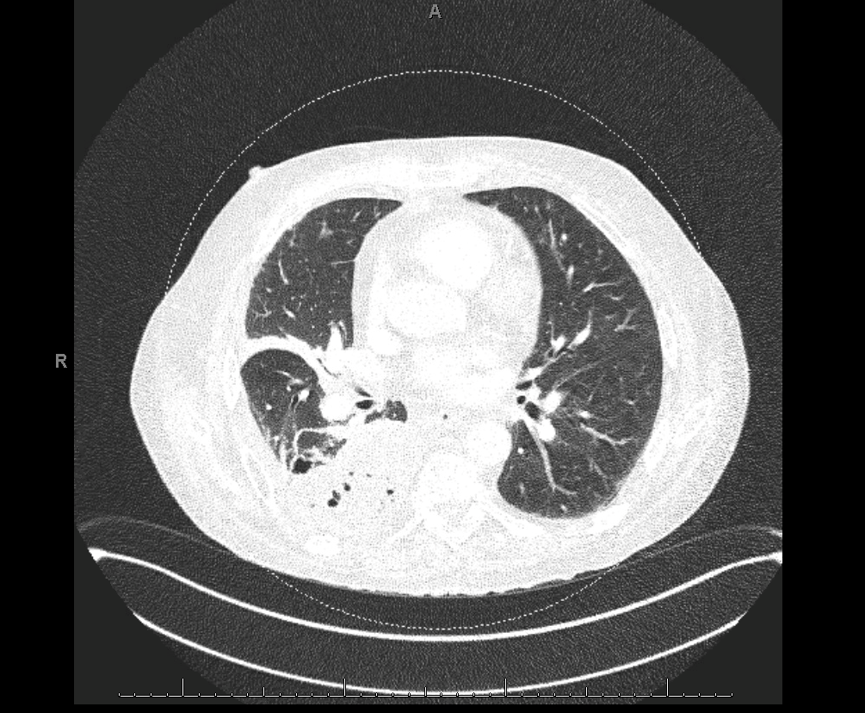
CT Chest (on 2nd admission): Interval reduction in size of the moderate right pleural effusion with adjacent compressive atelectasis. New gas within the pleural space probably entered at time of pigtail catheter placement. There is some overlying pleural enhancement, which can be secondary to the drainage procedure versus superimposed inflammation.
The POCUS team was consulted for consideration of diagnostic and therapeutic thoracentesis.
Case Continued
At time of our assessment, patient was noted to be hemodynamically stable and on room air. A lung ultrasound was performed:
R1
R3
R2

R6

Teaching Points
-
A thoracentesis can be diagnostic and/or therapeutic.
Diagnostic:
1. Pleural effusion of unclear etiologyTherapeutic
1. Dyspnea or hypoxia (attributed to the pleural effusion)
2. In the case of infected pleural fluid e.g. parapneumonic/empyema – drainage eliminates the source of infection and reservoirs of the infection -
Choosing between a thoracentesis or insertion of a pigtail catheter is dependent upon:
Patient-related factors
1. Effusion size: Large effusion may require pigtail insertion to allow serial drainage over a few days, max 1.5L/day
2. Necessity for complete drainage: Related to severity of symptoms, subsequent management plans
3. Rate of re-accumulation of fluid
4. Effusion type: loculated or free flowing
5. Need for additional therapeutics such as intrapleural tPA-DNaseNon-patient factors
1. Institutional factors
2. Operator preference
3. Availability of expertise -
Features that suggest an alternate etiology for the effusion:
1. Unilateral effusion
2. Bilateral effusions of significantly disparate sizes (especially if the effusion on the left is larger than on the right)
3. Symptoms of pleurisy or fever
4. Clinical suspicion for infection or cancer
5. No underlying cause for the volume overload (eg. Normal 2DE, stable renal function, no cirrhosis, no obvious precipitants)
6. Effusion appears complex on ultrasound

Case Continued
The patient underwent insertion of 14F pigtail at bedside, draining a small volume straw-coloured fluid. The pigtail catheter was connected to a Pleur-evac and allowed to drain to gravity.
Pleural fluid analysis:
- Cell count 75
- Hematocrit: <0.01 (serum Hct 0.27)
- pH 7.28
- Protein 35 (serum protein 73)
- LDH 1289 (serum LDH 311)
- cultures no growth -> unsurprising considering patient had received antibiotics over the past 2 weeks
- cytology: negative
A diagnosis of a complicated parapneumonic effusion was made. Only 100cc of fluid was drained overnight. Respirology recommended pigtail catheter flushes BID to maintain tube patency, and placing the tube on -20 cm H20 suction to promote drainage. He was given intrapleural tPA-DNase for 3 days, and the pigtail had good output (>2L) following lytic therapy.
CXR after lytic therapy

Case Conclusion
Respirology recommended a repeat CT chest with contrast to better characterize the pleural space, extent of loculations, and residual pleural effusion.
CT Chest (1 week post-pigtail insertion)
- Almost complete resolution of the fluid component and slight increase in the gas component of the small loculated right basal hydropneumothorax.
- Improvement in the atelectasis within the right lower lobe.
Once there was minimal drainage from pigtail (less than 100 cc/24 hrs), it was removed. Patient is planned to complete 6 weeks of antibiotic therapy (amox/clav).