
Hone your POCUS interpretation and clinical reasoning by working through the interactive cases below.
Case #10: I’d B-lining If I Knew (The Diagnosis): Consolidating Your Lung knowledge

Ms K. is a 62 year old female with alcoholic cirrhosis complicated by ascites, hypertension, and a history of a remote right MCA stroke. She presented to hospital with an UGIB secondary to NSAID use and gastroenteritis for which she received significant fluid resuscitation.
Following this, Ms K. developed hypoxemia (requiring 3L by NP) and one low grade temperature of 38.1C. She was also noted to have crepitations bilaterally on auscultation. CXR was reported as interstitial lung markings, likely in keeping with pulmonary edema. Creatinine was normal. The MRP team decided to start the patient on IV furosemide, and requested for a volume assessment by the POCUS team.
RIGHT UPPER ANTERIOR LUNG FIELD (R1)

RIGHT LUNG VIEWS
LEFT LUNG VIEWS
IVC, JVP, AND CARDIAC VIEWS (PLAX, APICAL 4-CHAMBER VIEW)

IVC in short-axis: small, ovoid, collapsible
LV and RV systolic function grossly normal, RV not enlarged, dilated LA
APICAL 5-CHAMBER VIEW FOR CALCULATION OF LVOT VTI

VTI correlates with stroke volume (and therefore cardiac output); normal VTI is >18
APICAL 4-CHAMBER VIEW TO CALCULATE E/e’ FOR LV DIASTOLIC DYSFUNCTION
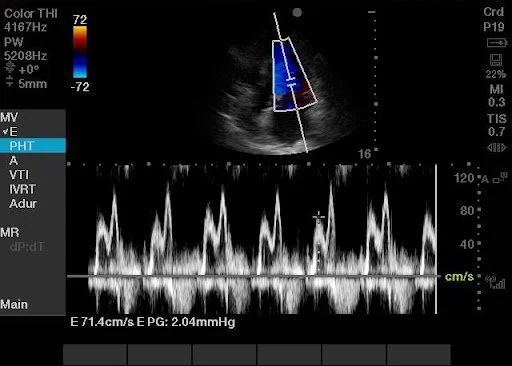
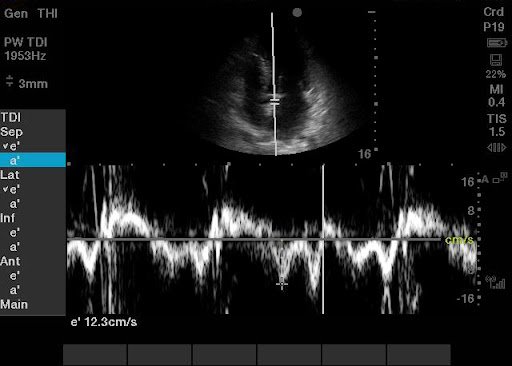
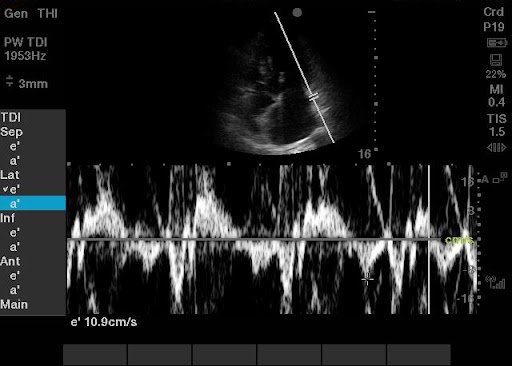
E/e’ = 71.4/11.6 = 6
This estimates left atrial pressure; E/e’ < 8 is considered normal LAP
CASE CONTINUATION
Based on the ultrasound findings, we recommended that the MRP team order a CT chest and more extensive respiratory infection work-up (sputum cultures, extended viral respiratory panel).

CT CHEST REPORT:
Confluent areas of ground-glass opacification with interlobular septal thickening involving entire left lung with patchy involvement of right lung. The findings are most suggestive of asymmetric acute lung injury/ diffuse alveolar damage.
CASE CONCLUSION
Patient had positive NAT for Human Metapneumovirus and positive sputum culture for Klebsiella pneumoniae. She improved on antibiotics and was discharged home when back on room air.